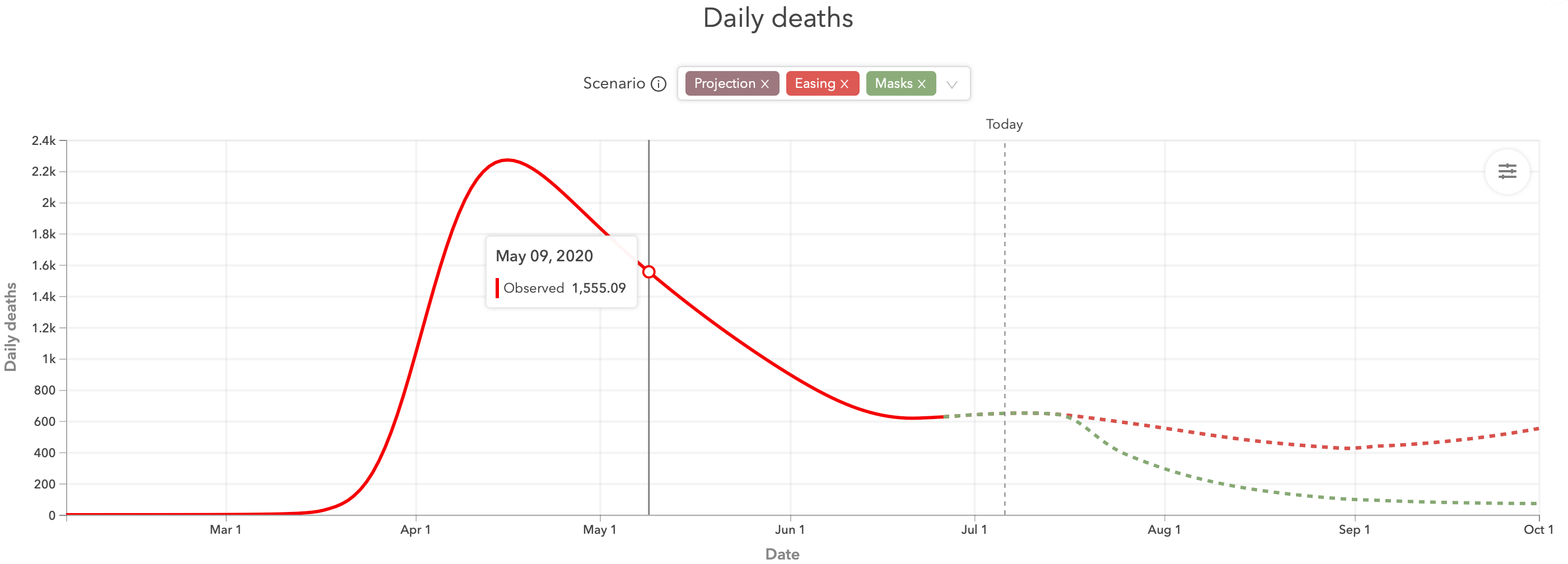
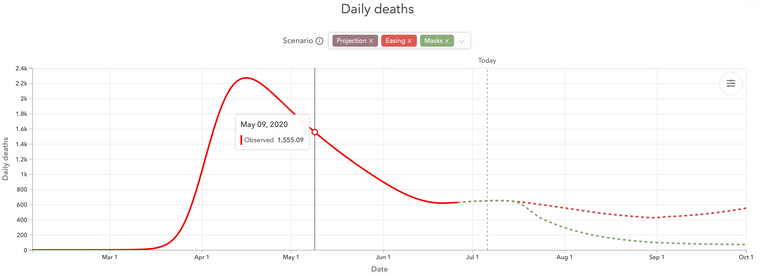
We haven't beat on the IHME model in a while
-
THey are not predicting a significant increase in the death rate even as the new case rate is doubling every 14 days.
Seems rather optimistic.
Person. Woman. Man. Camera. TV.
-
THey are not predicting a significant increase in the death rate even as the new case rate is doubling every 14 days.
Seems rather optimistic.
@jon-nyc said in We haven't beat on the IHME model in a while:
THey are not predicting a significant increase in the death rate even as the new case rate is doubling every 14 days.
Seems rather optimistic.
I've seen stories that the increased cases are not causing increased deaths because a) The virus is mutating to a less virulent strain (?) b) Increasing cases are among younger people who are more resilient (?) c) Admissions to hospitals because of SARS-CoV-2 are falling although the admissions to hospitals with SARS-CoV-2 are increasing.
-
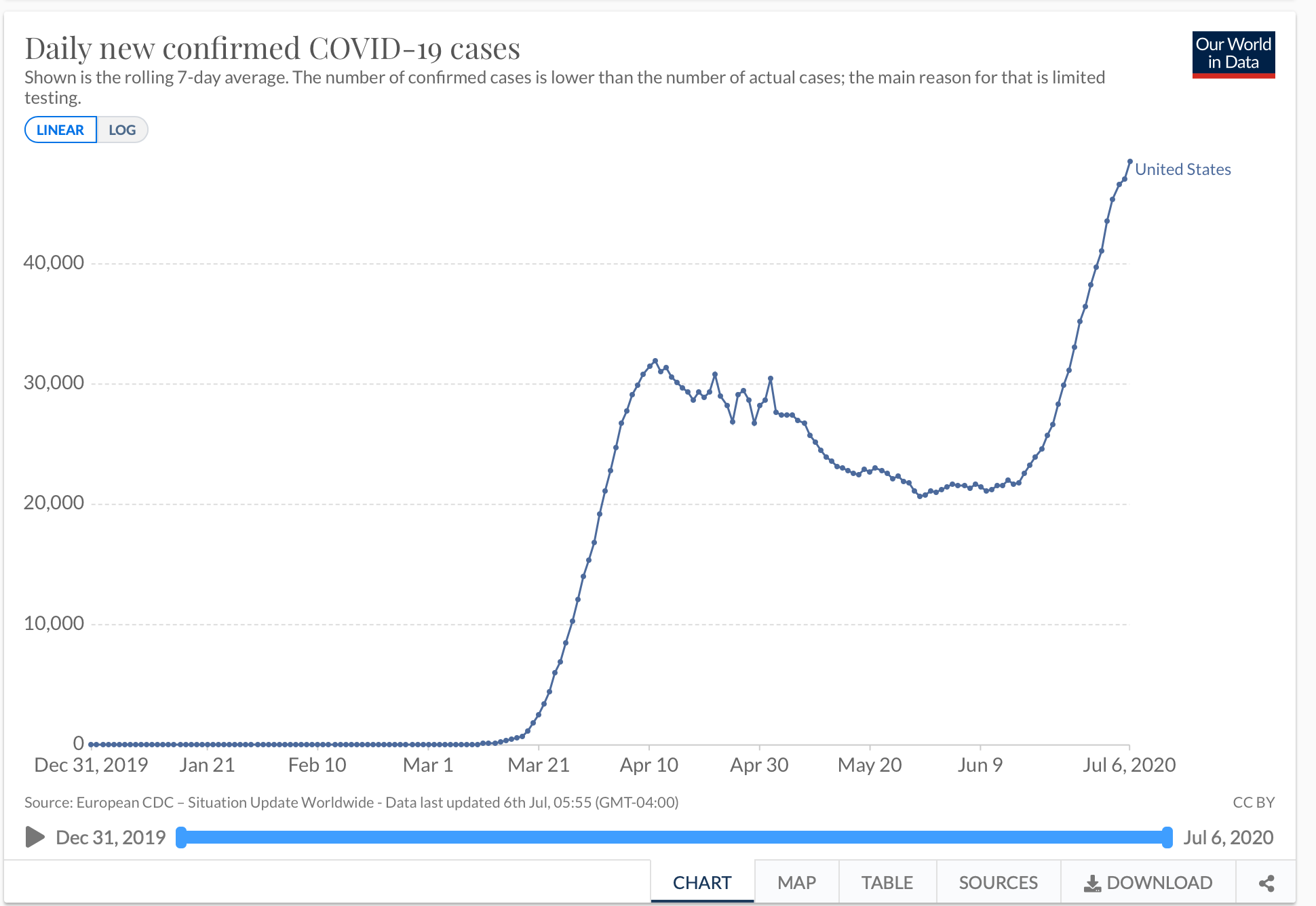
Doesn't it seem like about a zero % chance that daily deaths don't show an uptick in the face of that dramatic increase in cases? I don't mean a low chance, but literally no chance whatsoever?
Even if you posit the death rate has decreased since the first big wave, that would just mean the slope of the increase in deaths would be less than it would be if the death rate were the same as in April May. For the curve to remain flat the death rate would have to be continuously falling to offset the continuous growth in case rate.
-
It all depends on whether the vulnerable are more protected. Initially they were sitting ducks. Just think what NYC did to them.
Most nursing homes are experiencing very very low case loads, remember half of all deaths come from there...and many elderly live independently.
If the young aren’t spreading to the vulnerable and this plus the surge in testing is where the new cases are coming from just maybe deaths won’t soar. It’s not axiomatic that deaths will soar.
Maybe the IFR will finally show itself to be what the Diamond Princess told us many moons ago.
-
Again, a lower death rate wouldn't suffice. It would need to continuously fall over time. Like the death rate for people who contract the disease next week would have to be significantly lower than the death rate of people who contracted it the last week of June. Like much lower, less than half.
-
Again, a lower death rate wouldn't suffice. It would need to continuously fall over time. Like the death rate for people who contract the disease next week would have to be significantly lower than the death rate of people who contracted it the last week of June. Like much lower, less than half.
@jon-nyc said in We haven't beat on the IHME model in a while:
Again, a lower death rate wouldn't suffice. It would need to continuously fall over time. Like the death rate for people who contract the disease next week would have to be significantly lower than the death rate of people who contracted it the last week of June. Like much lower, less than half.
Well it’s about 5% right now if you look at confirmed cases and deaths. CDC says less than .5% possibly. Will be interesting to see how the data shakes out.
The best prediction is muddled.
-
I can't believe that at this late date you're still confused about CFR vs IFR.
But whatever.
What's your narrative as to why the people who contract it the week of July 12th will have a fatality rate ~1/2 that of those who contract it the week of June 29th?
Person. Woman. Man. Camera. TV.
-
I can't believe that at this late date you're still confused about CFR vs IFR.
But whatever.
What's your narrative as to why the people who contract it the week of July 12th will have a fatality rate ~1/2 that of those who contract it the week of June 29th?
@jon-nyc said in We haven't beat on the IHME model in a while:
I can't believe that at this late date you're still confused about CFR vs IFR.
But whatever.
What's your narrative as to why the people who contract it the week of July 12th will have a fatality rate ~1/2 that of those who contract it the week of June 29th?
I’m not confused, I’m doing a number of things at once which does lower ones IQ.
I am still waiting on the new CDC estimate that you lambasted and also your comments on the vulnerable being more protected. It’s the first thing I said when Covid came out that we had to do.
-
Things that I have not been able to find is what is the fatality rate and serious case rate for those over 65 alone, or 60-70, where I fall right in the middle. I have no feel for how many people my age get mild cases and how many serious or fatal.
@Mik said in We haven't beat on the IHME model in a while:
Things that I have not been able to find is what is the fatality rate and serious case rate for those over 65 alone, or 60-70, where I fall right in the middle. I have no feel for how many people my age get mild cases and how many serious or fatal.
My take is that the risk rises with age and comorbidity, although if I were 70 and healthy I wouldn’t be overly scared. Of course one could have the X factor for good or bad.
What has remained constant is the number of years of life lost due to Covid.
Harvard calculated at 1 year.
-
Bias is a fascinating thing. Regarding JB's old signature, we've certainly crossed the threshold.
-
Bias is a fascinating thing. Regarding JB's old signature, we've certainly crossed the threshold.
@Aqua-Letifer said in We haven't beat on the IHME model in a while:
Bias is a fascinating thing. Regarding JB's old signature, we've certainly crossed the threshold.
Everyone biased so far has had their comeuppance but I agree there is no loss of enthusiasm.
We were taught to rely on science. It’s been a rocky ride.
-
@Mik said in We haven't beat on the IHME model in a while:
Things that I have not been able to find is what is the fatality rate and serious case rate for those over 65 alone, or 60-70, where I fall right in the middle. I have no feel for how many people my age get mild cases and how many serious or fatal.
My take is that the risk rises with age and comorbidity, although if I were 70 and healthy I wouldn’t be overly scared. Of course one could have the X factor for good or bad.
What has remained constant is the number of years of life lost due to Covid.
Harvard calculated at 1 year.
@Loki said in We haven't beat on the IHME model in a while:
@Mik said in We haven't beat on the IHME model in a while:
Things that I have not been able to find is what is the fatality rate and serious case rate for those over 65 alone, or 60-70, where I fall right in the middle. I have no feel for how many people my age get mild cases and how many serious or fatal.
My take is that the risk rises with age and comorbidity, although if I were 70 and healthy I wouldn’t be overly scared. Of course one could have the X factor for good or bad.
What has remained constant is the number of years of life lost due to Covid.
Harvard calculated at 1 year.
How does that address my question?
-
I can't believe that at this late date you're still confused about CFR vs IFR.
But whatever.
What's your narrative as to why the people who contract it the week of July 12th will have a fatality rate ~1/2 that of those who contract it the week of June 29th?
@jon-nyc said in We haven't beat on the IHME model in a while:
I can't believe that at this late date you're still confused about CFR vs IFR.
But whatever.
I don't know what either CFR or IFR mean, I just haven't been worrying about it, really
Hasn't the amount of testing gone way up in the last few weeks?
Around here it has, there have been several local blood drive/testing events recently.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login