An avoidable medical inequity
-
How pulse oximeters work.
https://www.howequipmentworks.com/pulse_oximeter/
ETA:
This is a remarkable technology, when you think about it. When I started training, it was not available. By the time I finished training, it was available for the "sick patients." Within another 10 years, or so, it became the standard of care. Today, you can buy them at Walgreens.
Pulse oximetry and capnography are two of the biggest reasons why liability insurance for anesthesiologists plummeted in the late 20th century.
Sorry for the hijack...
-
I wonder if they'd find a sex disparity if they looked for it, since men have higher bone density.
After all, the disparity in covid deaths between the sexes dwarfs that observed between ethnic groups. One could imagine this being a contributing factor, at least at the margin.
-
Isn't this merely an education problem?
Once medical personell is aware of the problem, they can always interpret oximeter readings as "raw data" that has to be adjusted by a skin-color-dependent factor, similar to how weight alone is a bad measure of obesity and you need to factor in other things like height.
Having smarter devices would of course be more elegant, but I don't know how expensive and practical that would be.
-
Hm, if I understand correctly, the skin color aspect cannot be expressed by a simple linear relationship between reading and actual oxygen level. It's more like "the reading is inaccurate more frequently". Hmm...
-
Sure, ABG is the gold standard. But the whole purpose of pulse-ox is to be non-invasive for quick checks.
The devices are calibrated with a sample set. You can do multiple calibrations with distinct sets based on some objective (tech based) shade. measurement. You won’t get perfection but you could get better readings across the, uh, spectrum.
It’s not exact for whites now. There’s a percentage of whites where the difference between ABG and pulse-ox is enough to have clinically significant implications. It’s just that the percentage of blacks in the same category is larger.
Interestingly, in the study the best performing population (i.e., ABG/Pulse-ox readings were closest) were self declared ‘mixed race’. This probably arises from a calibrating data set that contained enough dark skinned samples to skew the results toward a middle ground shade of some sort.
-
Kind of funny to be typing all this is my hospital room and then the nurse come in to check my lilly-white vitals. Lol
@jon-nyc said in An avoidable medical inequity:
Kind of funny to be typing all this is my hospital room and then the nurse come in to check my lilly-white vitals. Lol
The question you have to ask yourself is do I feel privileged? Well, do ya, punk?
-
It's important to understand that the relationship between PaO2 (ABG) and SpO2 is anything but linear.
One can have serious hypoxemia (low PaO2) while still having a relatively "normal" SpO2.
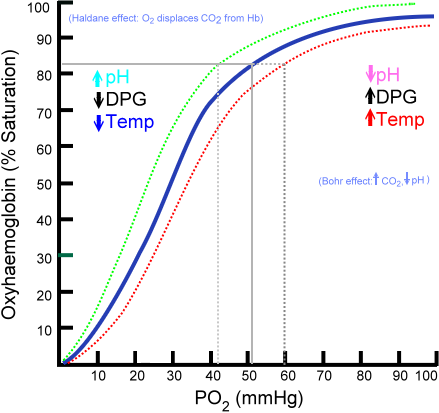
This is due to the unique structure of hemoglobin, with it's four components. As pH, Temperature, etc change, the affinity of oxygen to hemoglobin changes. As you can see from the picture, one can have a pretty significant hypoxemia (PaO2 of 70) with a relatively normal SpO2. As a point of fact, when blood returns to the heart to be re-oxygenated in the lungs, it's only given up about 25% of the oxygen it carried when it left.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login