My hospital(ist) rant

-
Is there enough for a
ambulance chaserlawyer to take up a case on contingency basis?Where else can you complain? Some sort of state regulatory body, professional ethics board?
Srsly, what’s the recourse for the regular people when sh!t like this happens to them?
@Axtremus said in My hospital(ist) rant:
Is there enough for a
ambulance chaserlawyer to take up a case on contingency basis?Where else can you complain? Some sort of state regulatory body, professional ethics board?
Srsly, what’s the recourse for the regular people when sh!t like this happens to them?
I think there's a malpractice claim in there, but harm would have to be proven. I know there's a CMS complaint (once they get the EOB showing that Medicare paid for care not given) in there, which should lead to a CMS investigation.
-
No harm was done.
You know the triad - injury, cause of injury, standard of care.
There's no malpractice here - it's just shitty medicine.
"Now look here, you Baltic gas passer... " - Mik, 6/14/08
The saying, "Lite is just one damn thing after another," is a gross understatement. The damn things overlap.
-
George, sorry to hear of this. You're juggling (or you're the glue?) holding lots of family together, and while there is no one better... it sucks it's on your shoulders. I was hopeful during the 2nd visit that she was seen so quickly as compared to the first hospital, but after she was brought to a room... nothing. Aside from rage, I am genuinely curious what their story is. Why wasn't she seen? Why was it written that she was?
-
George, sorry to hear of this. You're juggling (or you're the glue?) holding lots of family together, and while there is no one better... it sucks it's on your shoulders. I was hopeful during the 2nd visit that she was seen so quickly as compared to the first hospital, but after she was brought to a room... nothing. Aside from rage, I am genuinely curious what their story is. Why wasn't she seen? Why was it written that she was?
@89th said in My hospital(ist) rant:
I am genuinely curious what their story is. Why wasn't she seen? Why was it written that she was?
It's possible she was seen before I got there and the note was entered at 11:18.
But I doubt it.
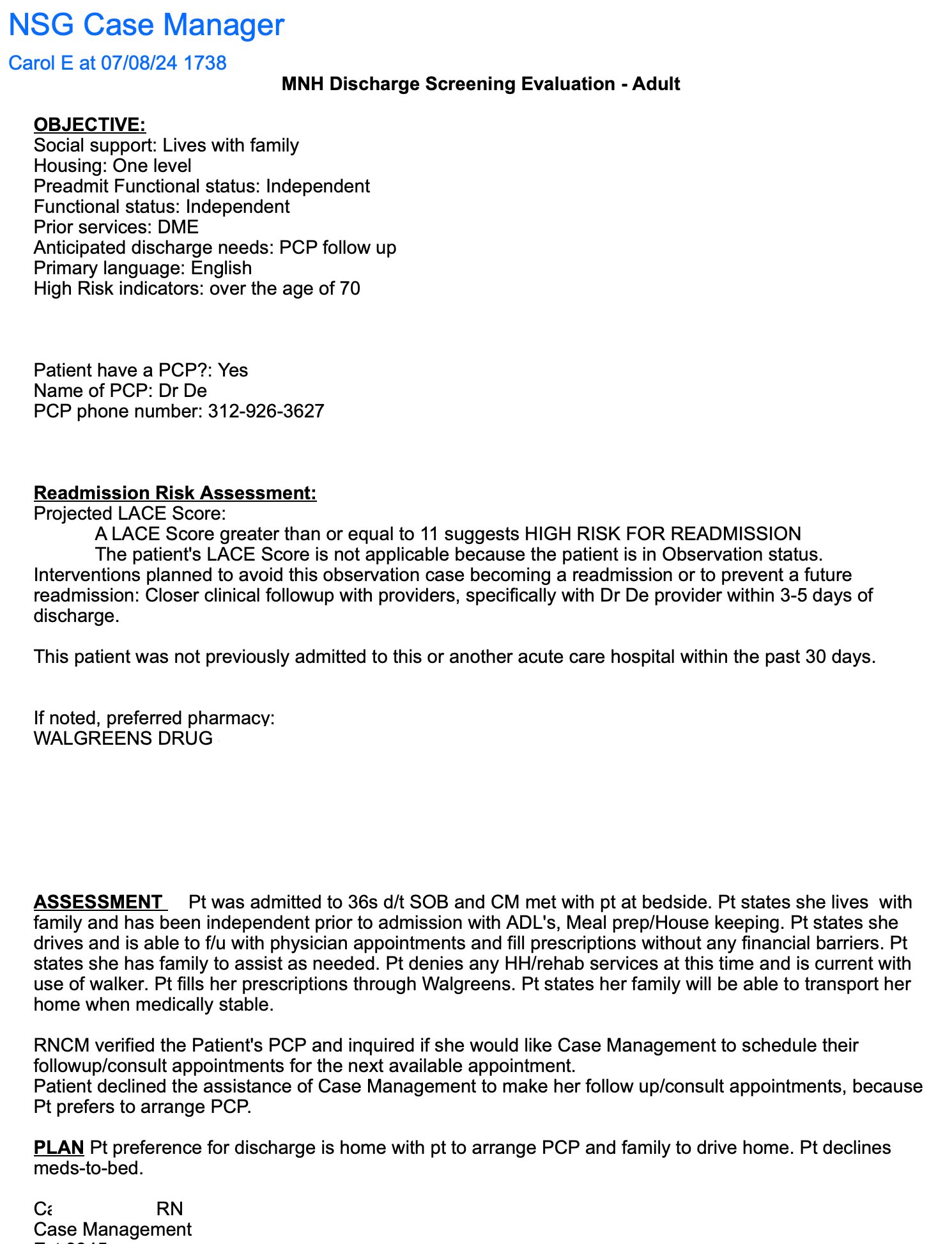
Also, the only person to speak to her before discharge was the floor nurse who assured us that all the prescriptions had been called in to Walgreens.
I was hopeful during the 2nd visit that she was seen so quickly as compared to the first hospital,
I really can't complain about the 1st hospital. We drove in, and they saw that she wasn't acutely ill, and had us in the waiting area. It was uncomfortable, but not horrible. The second place, she came in on a stretcher from the bambulance, on oxygen... triage is what they do.
-
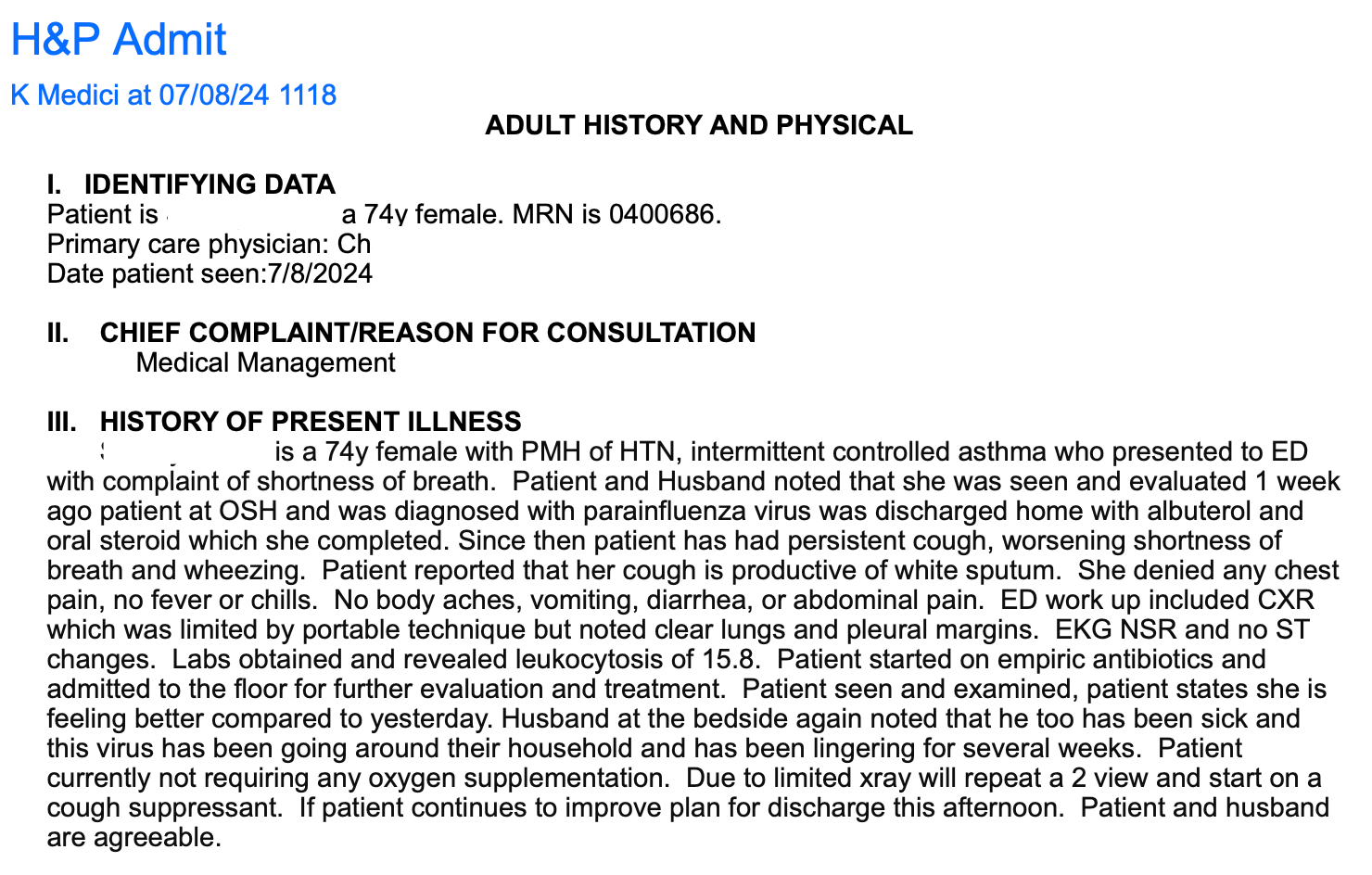
@George-K said in My hospital(ist) rant:
What really pisses me off is that the APRN notes that she saw Mrs. George at 11:18. I was there and it didn't happen. Perhaps she put the note in at that time and saw her earlier - I was there at 9:15.
Regardless, NO DOCTOR saw her.
No. Doctor. Saw. Her.
I am beyond furious. This is just shitty, shitty care.
No, that's negligence, malpractice and fraud.
@Jolly said in My hospital(ist) rant:
No, that's negligence, malpractice and fraud.
Yes. The doctor and nurse should be punished in some way for lying. It is fortunate that Mrs George did not have any bad consequences from their neglect, but if they did it once, they will probably do it again (or they probably have already done it before). Boo!!!!
-
No harm was done.
You know the triad - injury, cause of injury, standard of care.
There's no malpractice here - it's just shitty medicine.
@George-K said in My hospital(ist) rant:
No harm was done.
You know the triad - injury, cause of injury, standard of care.
There's no malpractice here - it's just shitty medicine.
Seems to me, care denied on purpose is care not given. Care not given results in a longer illness with the associated effects of such, which is harmful to the patient.
-
So sorry, George - this sounds like an awful experience
-
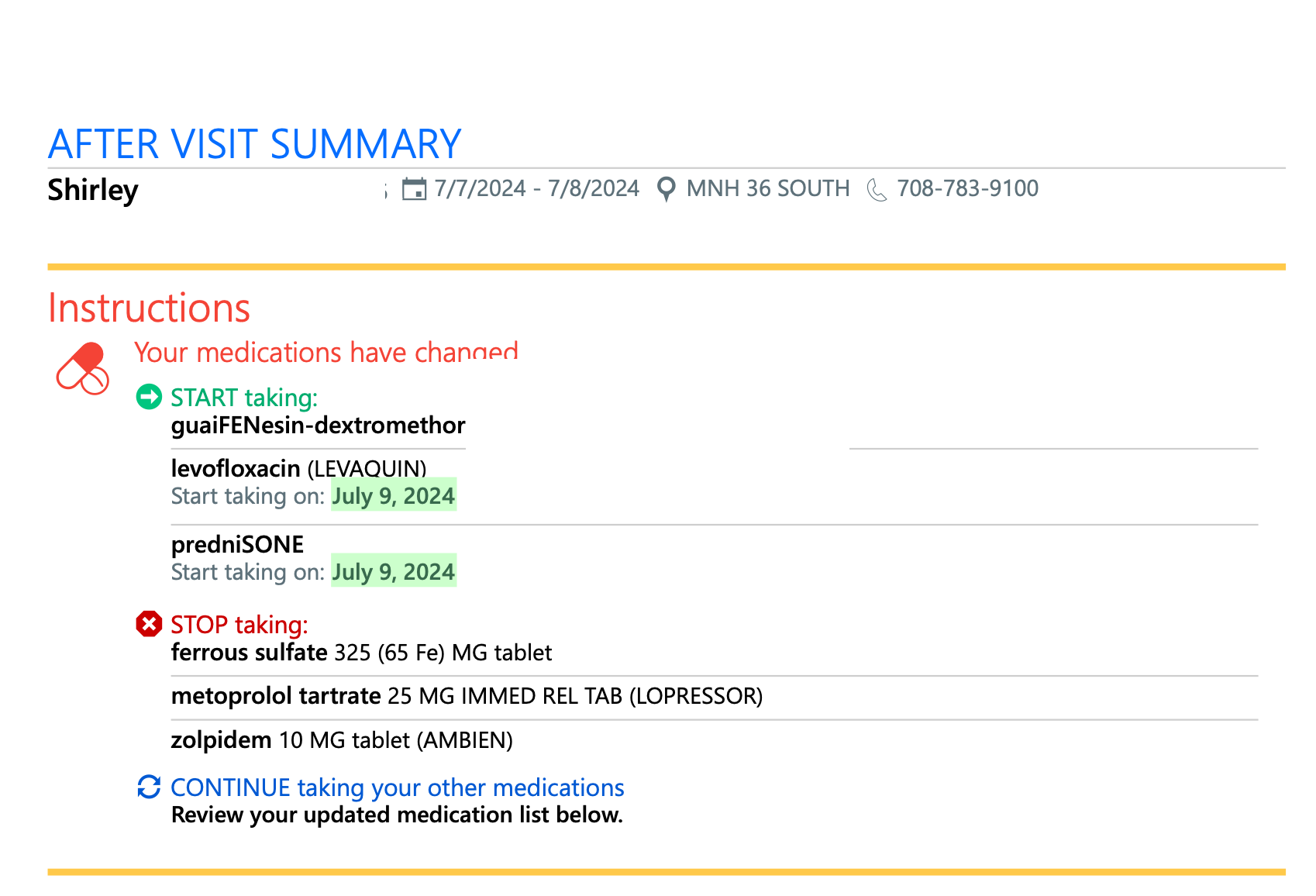
After spending the entire morning yesterday, trying to get these prescriptions filled from Hospital #2, I gave up.
I sent an email to her primary doc at northwestern explaining everything. I also called and explained the situation. I was told they'd try to get back to me same day. They didn't.
I got a call this AM (about 10 AM) and the nurse said that they are not comfortable prescribing the medication without seeing the patient - totally correct.
So, we have a video visit this PM at 2:40 for some steroids and antibiotics.
Well done...
-
Another note - hospital #2 has had a bad reputation for decades. In fact, it's been a standing joke of a place for a long time. When I went into private practice (at hospital #1) I was, overall, impressed with the quality of care. We had some surgeons come from #1 to do cases, and some of the internal medicine guys did as well. They were, for the most part, competent. Gradually, the more I worked with these guys, my impression of #2 started to change.
It can't be that bad, can it?
And then a large teaching hospital bought #2. Teaching hospital has a good reputation and some of my partners trained there. If you recall, our transportation options were teaching hospital (unknown duration of stay in ER) or #2, with the likelihood of being seen quickly higher.
It can't be that bad, can it?
Boy were we wrong. @kluurs can relay some stories about #2.
-
Back in the day (45 years ago), I worked for the National Cancer Institute. My position there let me know a lot about the various hospitals in the state. There were two where we just heard stories that meant we'd never let any family member go there. We had a staffer who lived near #2 - and would come in with horror stories.
Fast forward a couple of decades and my FIL was having a cardiac event, and MIL decides to drive him to #2. My spouse says "NO!!!" - take him to #1 - a major trauma center. But...it's easier to park at #2 - and "don't argue with me!" Get there - and while they didn't kill him, they came close. Fortunately, out-of-state BIL is a pathologist and called to say "get him the F out of #2" - so, he got transferred - went into arrest at #1 - but was successfully cared for - and lived 15+ more years.
Driving by #2 hospital a while back and noting the new Major Hospital Medical Center on the sign, I was wondering if this meant hope for hospital #2.
We had a B- kind of hospital in my town which become affiliated with a different Major Medical Center a while back - and has improved dramatically - to maybe an A-. I thought, well - maybe this means #2 may have improved. Based on George's experience, clearly, the 45 year reputation remains. If you get shot by a drive by while standing on the steps of that hospital, might be worth your while to Uber over to Hospital #1.
-
These sound like the horror stories you occasionally hear about British hospitals, which is normally blamed on the NHS being hopeless. My own personal experience with NHS urgent care was that it wasn't that bad at all (non-urgent care is a somewhat different matter, with waiting lists going back to the time of the dinosaurs), so maybe that is more hospital based as well.
-
Nurse called at noon, "Can you do a 2:40 appointment?"
"Sure! This is a telemedicine visit, right?"
"Er, no. You can't come in?
"Nah, too much of a trip and wait in the waiting room."
"No worries. 2:40 telemedicine it is."
Doc called about 40 min late (we would have been sitting in a waiting room all that time). Pleasant conversation, and she called in the scripts.
Easy.
She said that hospital #2 has a rep for being "sloppy."
-
-
Frown? Unless you're doing controlled substances I don't see why they would care.
Could always do doc-in-a-box a couple of days/week and pay for the expense. You'd be a helluva lot better than any NP could be.
I do keep trying to shove you back in through the EXIT door, don't I?

-
Frown? Unless you're doing controlled substances I don't see why they would care.
Could always do doc-in-a-box a couple of days/week and pay for the expense. You'd be a helluva lot better than any NP could be.
I do keep trying to shove you back in through the EXIT door, don't I?
@Jolly said in My hospital(ist) rant:
Could always do doc-in-a-box a couple of days/week and pay for the expense. You'd be a helluva lot better than any NP could be.
I do keep trying to shove you back in through the EXIT door, don't I?
Hard, hard nope.
Doing peds? Ladies with abdominal pain? Earaches? Runny noses?
Nope.
I could do simple ortho (put a cast on) and simple sutures. Nothing else.
-
@Jolly said in My hospital(ist) rant:
Could always do doc-in-a-box a couple of days/week and pay for the expense. You'd be a helluva lot better than any NP could be.
I do keep trying to shove you back in through the EXIT door, don't I?
Hard, hard nope.
Doing peds? Ladies with abdominal pain? Earaches? Runny noses?
Nope.
I could do simple ortho (put a cast on) and simple sutures. Nothing else.
@George-K said in My hospital(ist) rant:
@Jolly said in My hospital(ist) rant:
Could always do doc-in-a-box a couple of days/week and pay for the expense. You'd be a helluva lot better than any NP could be.
I do keep trying to shove you back in through the EXIT door, don't I?
Hard, hard nope.
Doing peds? Ladies with abdominal pain? Earaches? Runny noses?
Nope.
I could do simple ortho (put a cast on) and simple sutures. Nothing else.
Ok, you're hired!
-
One of the docs I used to work with, was our ED Director for several years, until he decided he actually wanted a life. He went into the urgent care biz. He does a pretty good job and runs some pretty good numbers, because he:
- Tries to staff his urgent cares (he has 4 or 5) with docs, if possible. If not, there is at least a couple of docs working at any given time. There is always a doc at his main place.
- His main urgent care has a Piccolo (great little chemistry machines, can do a full CMP/ liver enzymes/Troponin), a CBC machine with an automated diff, dipstick urinalysis and a bevy of LFT waived testing (flu/covid/strep/mono).
- His main urgent care also has an Xray and CT machine.
- Even his smaller shops have CBC, waived LFT, BMP, Troponin and xray capability.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login