Auxiliary Pump
-
A bit of background. "Cardiogenic shock" is what happens when heart muscle has been damaged by lack of blood flow, and the muscle can no longer pump enough blood to perfuse tissues. Kidney damage, cerebral ischemia etc are likely complications. It has a very high mortality, and if enough muscle is damaged, drugs to stimulate the heart and raise blood pressure can be ineffective.
Decades ago, a mechanical device was used to support the heart. A long balloon (about 10-12 inches long) was inserted into the aorta, downstream from the heart. The balloon would inflate and deflate in synchrony with the heart - deflating when the heart contracts (lowering the pressure head against which the heart has to pump) and inflating during relaxation causing blood to flow backward, increasing flow through the coronary arteries. It was a mainstay of therapy, but had its own set of complications. At first, just putting it in was a big deal, but that tech improved.
Now there's a new device. It's basically a propeller inserted in the vasculature to improve blood flow. It looks like it's easier to insert than a balloon, and compared to "standard therapy" with drugs, it appears to have a significant benefit in survival at 180 days.
Cool stuff.
Link to video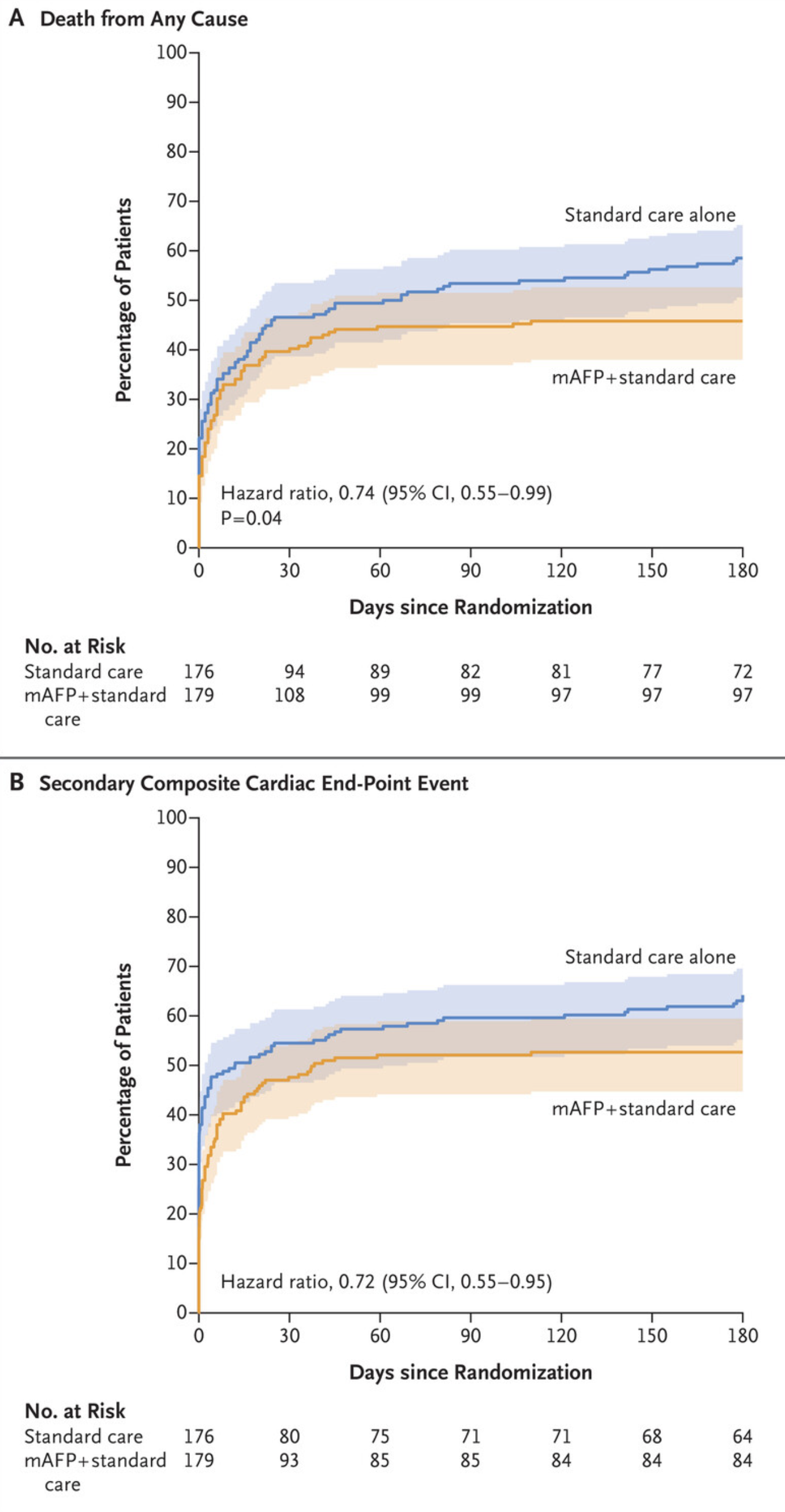
-
Getting into the weeds a bit.
The IABP (Intra Aortic Balloon Pump) is a notoriously tricky device to operate. The timing of inflation and deflation have to be adjusted very, VERY, precisely. If you fuck it up, someone's heart attack might very well get bigger, and that would be the best outcome.
Mrs. George, in another life, taught some courses on how to manage the IABP in the ICU.
If we had trouble weaning an open heart patient from the pump, the surgeon would insert an IABP to "unload" the heart and hopefully get the patient to the ICU.
In the "bad old days" inserting an IABP was a big deal. Surgeon would make an incision in the groin and find the femoral artery. He would then take a piece of dacron tubing, about ¾" in diameter and sew its end to an incision in the femoral artery. Then, the IABP would be inserted through the Dacron. Taking the IABP out was another trip to the OR - had to remove the graft on the femoral artery and then close the artery.
Eventually, the tech matured so that the IABP could be inserted percutaneously. Made a huge difference.
https://en.wikipedia.org/wiki/Intra-aortic_balloon_pump
Link to video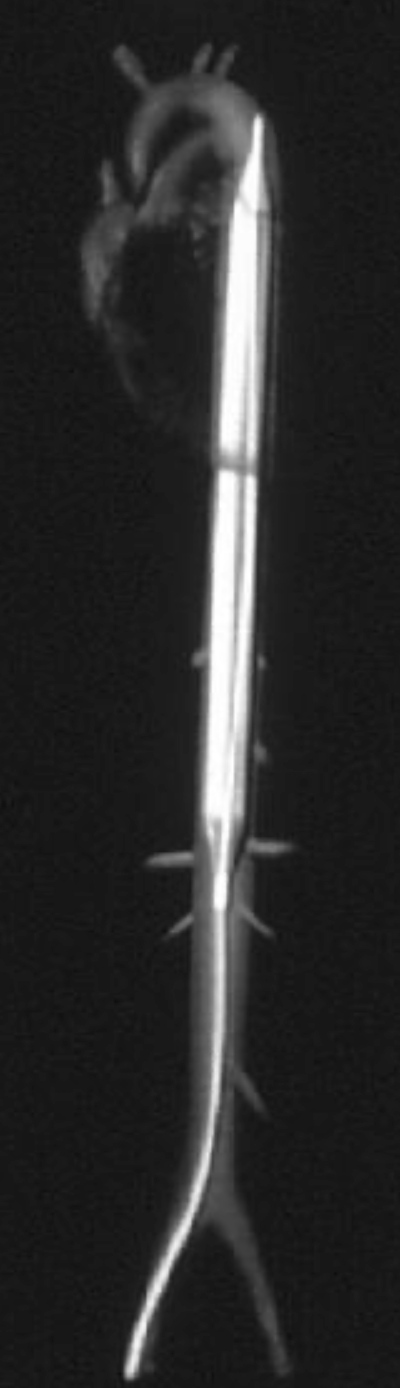
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login