Nurse Practitioners
-
Nurse practitioners (NPs) delivering emergency care without physician supervision or collaboration in the Veterans Health Administration (VHA) increase lengths of stay by 11% and raise 30-day preventable hospitalizations by 20% compared with emergency physicians, says a working paper published by the National Bureau of Economic Research.
That higher preventable hospitalization rate “may reflect two possibilities,” says the working paper, written by David Chan, MD, PhD, associate professor of health policy at Stanford University School of Medicine, and Yiqun Chen, PhD, assistant professor of economics at the University of Illinois at Chicago.
One is that “NPs have poorer decision-making over whom to admit to the hospital, resulting in underadmission of patients who should have been admitted and a net increase in return hospitalizations, despite NPs using longer lengths of stay to evaluate patients’ need for hospital admission.”
The other possibility is that “NPs produce lower quality of care conditional on admitting decisions, despite spending more resources on treating the patient (as measured by costs of the ED care). Both possibilities imply lower skill of NPs relative to physicians.”
Patients deserve greater clarity on who is a physician—and who isn’t
Overall, the study shows that NPs increase the cost of ED care by 7%, or about $66 per patient. Increasing the number of NPs on duty to decrease wait times raised total health care spending by 15%, or $238 per case—not including the cost of additional NP salaries. In all, assigning 25% of emergency cases to NPs results in net costs of $74 million annually for the VHA.“Increasing the number of NPs on duty decreases wait times, but increases resource utilization and adverse outcomes,” says the working paper. The primary contributor these higher costs was “lower productivity”—that is, NPs were likelier to order tests such as X-rays and CT scans and seek formal consults than were emergency physicians.
Patients deserve care led by physicians—the most highly educated, trained and skilled health professionals. That is why the AMA vigorously defends the practice of medicine against scope-of-practice expansions that threaten patient safety as part of the AMA Recovery Plan for America’s Physicians.
Unlike other research comparing the performance of physicians and nonphysicians and the impact of scope-of-practice expansions on cost and quality of care, this economic study looks beyond correlation by using a high-quality causal analysis.
And while many other studies attempt to draw comparisons based on NPs or other nonphysicians who are actually practicing in collaborative arrangements with physicians, this study leverages data from a time—2017 to 2020, right before the pandemic—in which NPs within the VHA were truly practicing without physician supervision.
The study found the physician-NP gap on cost and quality grew with patient complexity, with NPs being more likely to admit to the hospital patients with complex or severe conditions. The effect of NPs on lengths of stay and medical costs also rose with the complexity of the patient’s condition.
Physicians complete between 10,000 and 16,000 hours of clinical education and training—four years in medical school and another three to seven years of residency training. By comparison, NPs complete between 500–720 hours of clinical training during two or three years of graduate-level education. Learn more with the AMA about why education matters in scope of practice.
A study by researchers from Johns Hopkins University, the University of New Mexico and other institutions, found that few NPs are certified to deliver emergency care and that NP qualifications to practice in emergency departments vary widely among states.
My encounters with NPs have been mixed. I'm fortunate to understand that when they don't know something, I get it and can seek other advice. Most people aren't that lucky.
See my comments about my facial cellulitis as an example,
"Now look here, you Baltic gas passer... " - Mik, 6/14/08
The saying, "Lite is just one damn thing after another," is a gross understatement. The damn things overlap.
-
I've had similar experiences with them. Some are good, some aren't. What you have to hope for is you get lucky, and that's not acceptable.
@Mik said in Nurse Practitioners:
I've had similar experiences with them. Some are good, some aren't. What you have to hope for is you get lucky, and that's not acceptable.
Right. When I had my parotid infection, I knew she was wrong in the diagnosis, but right in the treatment. I was content to walk out with a prescription for Augmentin. I saw an ENT the next day.
Now, if I had been having chest pain...
-
Nurse practitioners (NPs) delivering emergency care without physician supervision or collaboration in the Veterans Health Administration (VHA) increase lengths of stay by 11% and raise 30-day preventable hospitalizations by 20% compared with emergency physicians, says a working paper published by the National Bureau of Economic Research.
That higher preventable hospitalization rate “may reflect two possibilities,” says the working paper, written by David Chan, MD, PhD, associate professor of health policy at Stanford University School of Medicine, and Yiqun Chen, PhD, assistant professor of economics at the University of Illinois at Chicago.
One is that “NPs have poorer decision-making over whom to admit to the hospital, resulting in underadmission of patients who should have been admitted and a net increase in return hospitalizations, despite NPs using longer lengths of stay to evaluate patients’ need for hospital admission.”
The other possibility is that “NPs produce lower quality of care conditional on admitting decisions, despite spending more resources on treating the patient (as measured by costs of the ED care). Both possibilities imply lower skill of NPs relative to physicians.”
Patients deserve greater clarity on who is a physician—and who isn’t
Overall, the study shows that NPs increase the cost of ED care by 7%, or about $66 per patient. Increasing the number of NPs on duty to decrease wait times raised total health care spending by 15%, or $238 per case—not including the cost of additional NP salaries. In all, assigning 25% of emergency cases to NPs results in net costs of $74 million annually for the VHA.“Increasing the number of NPs on duty decreases wait times, but increases resource utilization and adverse outcomes,” says the working paper. The primary contributor these higher costs was “lower productivity”—that is, NPs were likelier to order tests such as X-rays and CT scans and seek formal consults than were emergency physicians.
Patients deserve care led by physicians—the most highly educated, trained and skilled health professionals. That is why the AMA vigorously defends the practice of medicine against scope-of-practice expansions that threaten patient safety as part of the AMA Recovery Plan for America’s Physicians.
Unlike other research comparing the performance of physicians and nonphysicians and the impact of scope-of-practice expansions on cost and quality of care, this economic study looks beyond correlation by using a high-quality causal analysis.
And while many other studies attempt to draw comparisons based on NPs or other nonphysicians who are actually practicing in collaborative arrangements with physicians, this study leverages data from a time—2017 to 2020, right before the pandemic—in which NPs within the VHA were truly practicing without physician supervision.
The study found the physician-NP gap on cost and quality grew with patient complexity, with NPs being more likely to admit to the hospital patients with complex or severe conditions. The effect of NPs on lengths of stay and medical costs also rose with the complexity of the patient’s condition.
Physicians complete between 10,000 and 16,000 hours of clinical education and training—four years in medical school and another three to seven years of residency training. By comparison, NPs complete between 500–720 hours of clinical training during two or three years of graduate-level education. Learn more with the AMA about why education matters in scope of practice.
A study by researchers from Johns Hopkins University, the University of New Mexico and other institutions, found that few NPs are certified to deliver emergency care and that NP qualifications to practice in emergency departments vary widely among states.
My encounters with NPs have been mixed. I'm fortunate to understand that when they don't know something, I get it and can seek other advice. Most people aren't that lucky.
See my comments about my facial cellulitis as an example,
@George-K said in Nurse Practitioners:
… imply lower skill of NPs relative to physicians.”
Well, duh!
Overall, the study shows that NPs increase the cost of ED care by 7%, or about $66 per patient. Increasing the number of NPs on duty to decrease wait times raised total health care spending by 15%, or $238 per case—not including the cost of additional NP salaries.
Not sure what that means. The +7%/$66 per patient number, what does that compare to? Providing the same care without using any RN at all? If 7%=$66, then 15% would be $141 rather than $238, so I am not sure what are being compared here.
Patients deserve care led by physicians—the most highly educated, trained and skilled health professionals.
Yes, now train more of them and/or admit more of them from elsewhere.
Unlike other research comparing the performance of physicians and nonphysicians and the impact of scope-of-practice expansions on cost and quality of care, this economic study looks beyond correlation by using a high-quality causal analysis.
Good stuff, this sort of analysis is important.
-
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
-
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
@taiwan_girl said in Nurse Practitioners:
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
Fine for taking your weight, BP, etc. That's about it.
-
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
@taiwan_girl said in Nurse Practitioners:
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
A PA is different from a NP.
A PA works in conjunction with one (or a group of) physician. S/he is the "right hand" that "takes care of business." The important word is "assistant." For example, when I saw the ortho guy about my tennis elbow a few months ago, he made the diagnosis, and the PA did the injection. Similarly, when I was doing heart surgery, the PA was the one to collate all the lab work, report to the surgeon, institute therapy after consultation, pull chest tubes, etc. The PA is the "eyes, ears and hands" of the doc. Of course my experience with non-surgical PAs is limited.
The NP is whole 'nother thing. The NP is trained to work pretty independently. The important word here is "practitioner." They can diagnose, treat and prescribe. In some jurisdictions, they must work under the aegis of a physician. The doc, in these cases, carries the ultimate responsibility and, if things go bad, the ultimate liability. However, in other cases, they practice independently. The article I cited seems to point to that case. The Veteran's Hospitals have been moving to more independent practice by NPs.
-
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
@taiwan_girl said in Nurse Practitioners:
For our medical people here, what do you think of Physician Assistant (PA)? I know that they are also becoming popular in the US.
The lines do blur, but Dr. K is correct, IME.
Here's an overview:
https://www.lsuhs.edu/departments/allied-health-professions-departments/physician-assistant
-
The problem with PAs is that they tend to be one-trick ponies. During school, they learn the jargon, basic physiology, pharmacology, etc.
But, for the most part, it's OJT - you learn to do what your supervising doc does, be it heart surgery or orthopedics. I'd guess that the ortho PA who injected my elbow would be lost in the heart room and the ICU. She would learn, probably quickly, but it's still OJT.
The NPs claim to have a broader range of practice and that might be true.
-
When my wife had gallstones, she saw several doctors. All said it wasn't gallstones.
On our way back from visiting my folks, she had a bad attack. Had to stop at an ER. Doc thought it was a freaking urinary infection, but he left. PA came in and thought, y'know, very well could be gallstones.
It was, and her gallbladder was in a very bad way. They took it out that night. Doc who did it told her afterward that it was pretty gnarly and why didn't she see someone sooner? You really shouldn't wait to see someone if you have abdominal pain bler der etc.
Please love yourself.
-
I can't find the source for this, but it doesn't strain credulity.
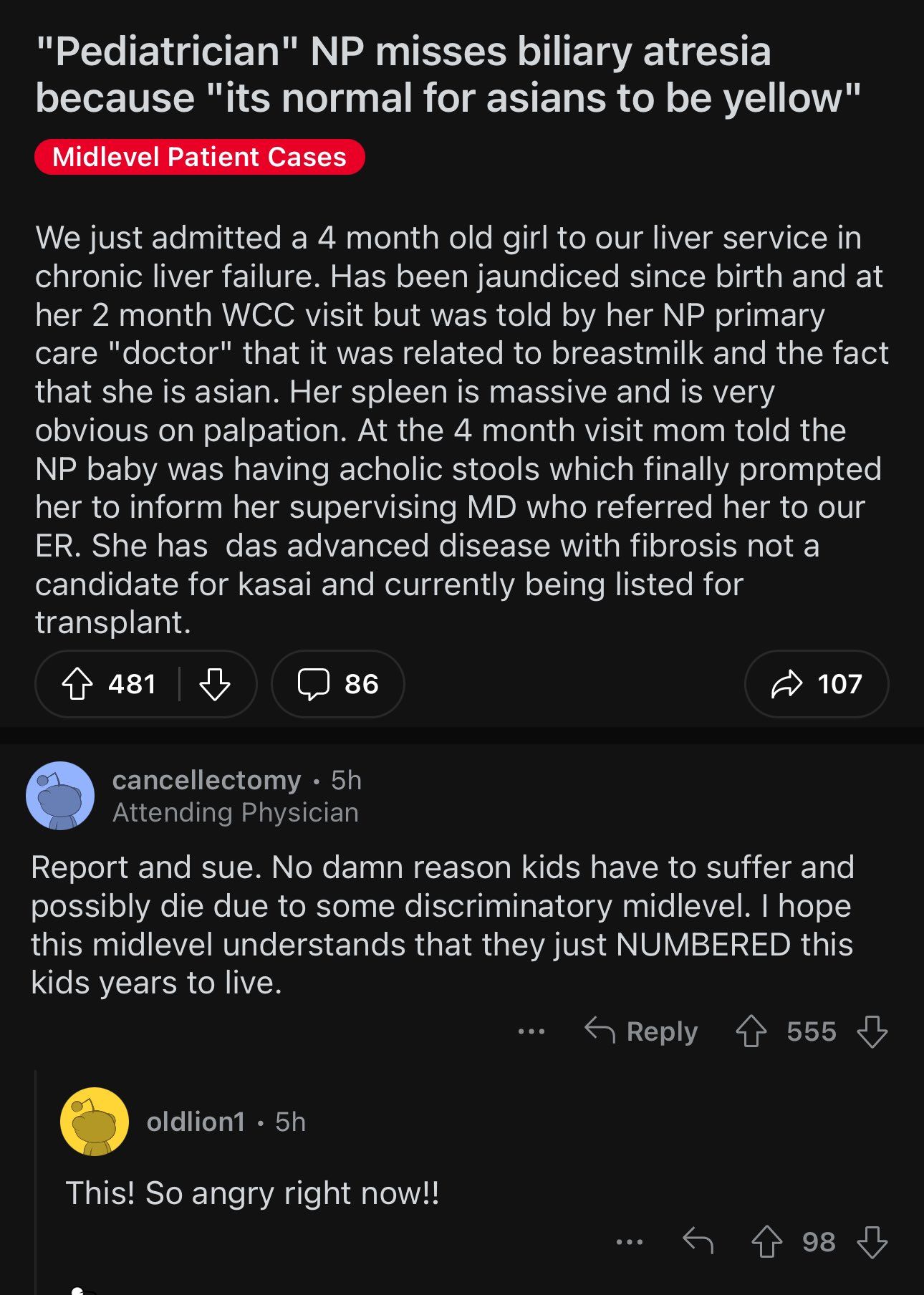
https://www.reddit.com/r/Noctor/comments/1f0aw7r/pediatrician_np_misses_biliary_atresia_because/
-
"Now look here, you Baltic gas passer... " - Mik, 6/14/08
The saying, "Lite is just one damn thing after another," is a gross understatement. The damn things overlap.
-
When my wife had gallstones, she saw several doctors. All said it wasn't gallstones.
On our way back from visiting my folks, she had a bad attack. Had to stop at an ER. Doc thought it was a freaking urinary infection, but he left. PA came in and thought, y'know, very well could be gallstones.
It was, and her gallbladder was in a very bad way. They took it out that night. Doc who did it told her afterward that it was pretty gnarly and why didn't she see someone sooner? You really shouldn't wait to see someone if you have abdominal pain bler der etc.
@Aqua-Letifer said in Nurse Practitioners:
When my wife had gallstones, she saw several doctors. All said it wasn't gallstones.
On our way back from visiting my folks, she had a bad attack. Had to stop at an ER. Doc thought it was a freaking urinary infection, but he left. PA came in and thought, y'know, very well could be gallstones.
It was, and her gallbladder was in a very bad way. They took it out that night. Doc who did it told her afterward that it was pretty gnarly and why didn't she see someone sooner? You really shouldn't wait to see someone if you have abdominal pain bler der etc.
HIDA scan. Insurance probably didn't want to pay for it.
-
@George-K said in Nurse Practitioners:
@Mik said in Nurse Practitioners:
Lord.
Read the reddit thread for more stories.
I don't know why we're getting on nurses in this thread. Roughly half of all the doctors I've ever had to deal with have been absolute dipshits. There's nothing special about nurses that make them especially susceptible to dipshittery.
-
@George-K said in Nurse Practitioners:
@Mik said in Nurse Practitioners:
Lord.
Read the reddit thread for more stories.
I don't know why we're getting on nurses in this thread. Roughly half of all the doctors I've ever had to deal with have been absolute dipshits. There's nothing special about nurses that make them especially susceptible to dipshittery.
@Aqua-Letifer said in Nurse Practitioners:
@George-K said in Nurse Practitioners:
@Mik said in Nurse Practitioners:
Lord.
Read the reddit thread for more stories.
I don't know why we're getting on nurses in this thread. Roughly half of all the doctors I've ever had to deal with have been absolute dipshits. There's nothing special about nurses that make them especially susceptible to dipshittery.
It's not nurses per se. It's the encroachment of nurses into where they have no business, even with additional training. I know some very good nurses. I even know some pretty decent NP's and PA's. But they're NOT doctors. They don't have the education, the training or the experience.
Not to say there are not bad physicians. Anybody with a passing knowledge of the medical system knows that.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login