Bullet
-
http://www.thomas-morris.uk/a-tale-of-two-inventions/
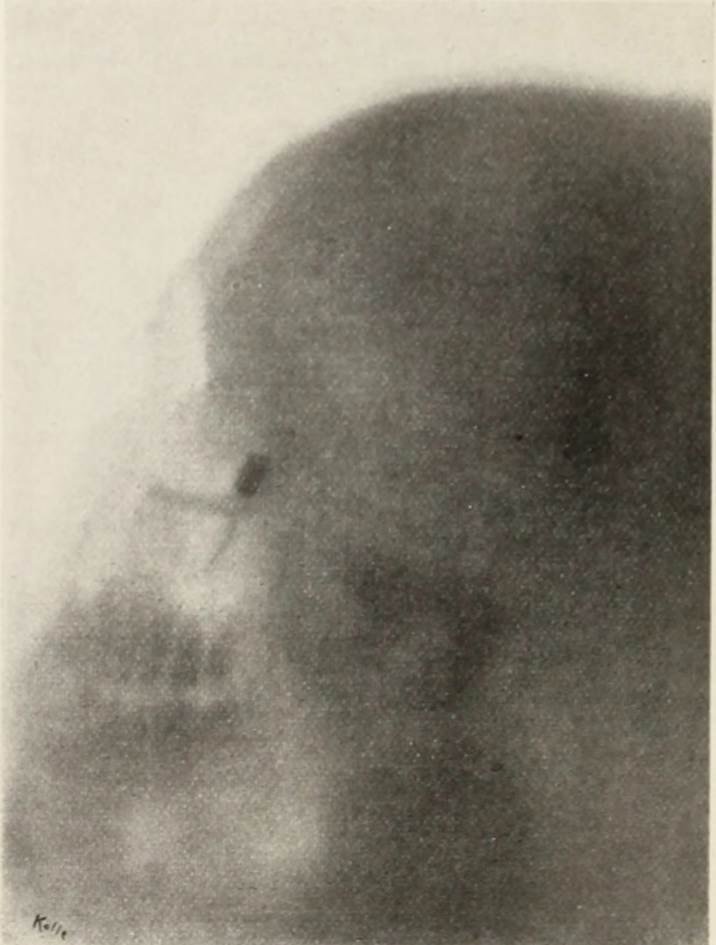
X-ray taken on October 13 1896, showing side view of patient’s skull and bullet lodged in region of eye socket.The X-ray gave Dr Fowler a very good idea of where to look for the bullet, although as it was a flat two-dimensional image it did not allow him to localise it precisely. On 17 October the patient was anaesthetised with ether and the surgeon made his search for the missing bullet.
The pointed telephonic probe, which was blunted so that it could not penetrate a vessel, and yet be sufficiently wedge-shaped to penetrate muscular and fascial structures, was passed through a small incision in the skin made as nearly as possible at a point opposite to the supposed location of the ball. A systematic exploration of the zygomatic and adjoining portion of the temporal fossa was then made in all available directions.
The zygomatic is the cheekbone, around the side and base of the eye socket. The temporal fossa is the side of the skull, around the temple.
The results of these excursions with the telephonic probe in the soft parts of the neighborhood were negative. The instrument was then introduced at the outer canthus, and the external and inferior aspects of the globe also explored, but with no result.
The outer canthus is the outer corner of the eye. The surgery now became more complex, as Dr Fowler decided to make an incision through the cheekbone and explore behind it.
The parts thus brought within reach were now submitted to a most searching investigation with the probe, but nothing was found.
Still nothing! So the surgeon decided to investigate the eye socket more thoroughly.
The margin of the outer wall of the orbit was now chiseled away until free access to that cavity was obtained, when the probe was made to explore all portions of the orbit outside of the globe. This extension of the exploratory operative procedure, however, was without result.
A lesser surgeon might have given up at this point. But Dr Fowler was not to be defeated.
If the results of the Röntgen-ray picture were not to be doubted, and the symptom of double blindness was not misleading, in the absence of all evidences of intracranial injury there was but one other place remaining to be subjected to investigation, and that was the globe itself.
By which he means the interior of the eyeball.
I therefore carefully introduced the telephonic probe through the sclerotic at the site of the gap left by chiseling away the orbital margin, when the presence of the bullet as it came into contact with the end of the probe was at once announced by the characteristic “click” in the telephone receiver.
What a moment! The ‘sclerotic’, now more usually known as the sclera, is the tough white outer layer of the eye.
A half-inch incision was then made through the sclerotic coat at the site of the puncture made by the probe, and the bullet, bearing marks of its passage through the bony parts, removed.
The surgeon then repaired the bone flap he had made earlier, and sutured the soft tissues above it. And that was it: job done.
Rapid healing followed, and the patient was discharged from the hospital at the end of a fortnight.
-
http://www.thomas-morris.uk/a-tale-of-two-inventions/
X-ray taken on October 13 1896, showing side view of patient’s skull and bullet lodged in region of eye socket.The X-ray gave Dr Fowler a very good idea of where to look for the bullet, although as it was a flat two-dimensional image it did not allow him to localise it precisely. On 17 October the patient was anaesthetised with ether and the surgeon made his search for the missing bullet.
The pointed telephonic probe, which was blunted so that it could not penetrate a vessel, and yet be sufficiently wedge-shaped to penetrate muscular and fascial structures, was passed through a small incision in the skin made as nearly as possible at a point opposite to the supposed location of the ball. A systematic exploration of the zygomatic and adjoining portion of the temporal fossa was then made in all available directions.
The zygomatic is the cheekbone, around the side and base of the eye socket. The temporal fossa is the side of the skull, around the temple.
The results of these excursions with the telephonic probe in the soft parts of the neighborhood were negative. The instrument was then introduced at the outer canthus, and the external and inferior aspects of the globe also explored, but with no result.
The outer canthus is the outer corner of the eye. The surgery now became more complex, as Dr Fowler decided to make an incision through the cheekbone and explore behind it.
The parts thus brought within reach were now submitted to a most searching investigation with the probe, but nothing was found.
Still nothing! So the surgeon decided to investigate the eye socket more thoroughly.
The margin of the outer wall of the orbit was now chiseled away until free access to that cavity was obtained, when the probe was made to explore all portions of the orbit outside of the globe. This extension of the exploratory operative procedure, however, was without result.
A lesser surgeon might have given up at this point. But Dr Fowler was not to be defeated.
If the results of the Röntgen-ray picture were not to be doubted, and the symptom of double blindness was not misleading, in the absence of all evidences of intracranial injury there was but one other place remaining to be subjected to investigation, and that was the globe itself.
By which he means the interior of the eyeball.
I therefore carefully introduced the telephonic probe through the sclerotic at the site of the gap left by chiseling away the orbital margin, when the presence of the bullet as it came into contact with the end of the probe was at once announced by the characteristic “click” in the telephone receiver.
What a moment! The ‘sclerotic’, now more usually known as the sclera, is the tough white outer layer of the eye.
A half-inch incision was then made through the sclerotic coat at the site of the puncture made by the probe, and the bullet, bearing marks of its passage through the bony parts, removed.
The surgeon then repaired the bone flap he had made earlier, and sutured the soft tissues above it. And that was it: job done.
Rapid healing followed, and the patient was discharged from the hospital at the end of a fortnight.
So why didn’t they do XYZ axial X-rays to find the bullet rather than jabbing around in his cranium?
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login